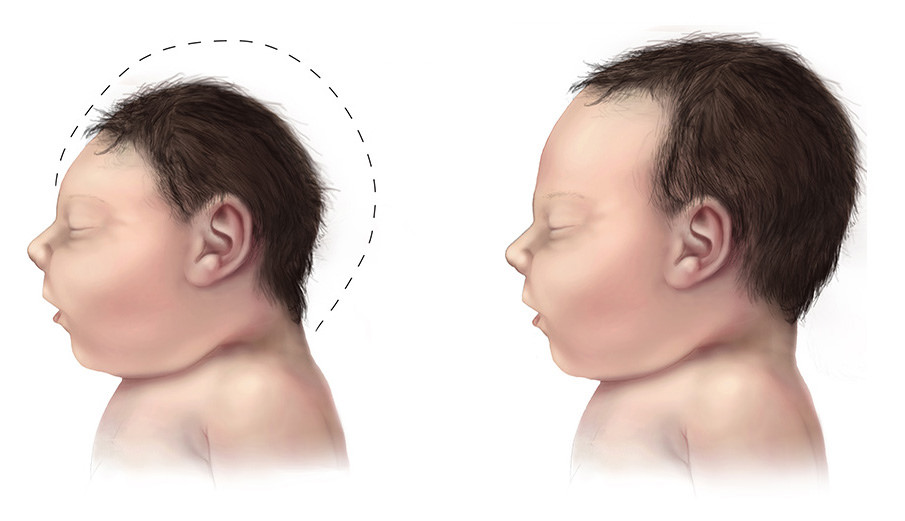
Zika Virus infection is a disease caused by the Zika virus spread mostly by the bite of an infected Aedes species mosquito. This infection can also be passed from a pregnant woman to her foetus and is dangerous for new-borns as it can result in foetal microcephaly. Foetal microcephaly is characterised by smaller head and brain size and can cause problems such as seizures, developmental delay, difficulty in movement and balance, speech defects and vision defects.

On the 3rd of November 2018, the Ministry of Health and Family Welfare (MoHFW), in a press release titled “Zika Virus strain that causes microcephaly not found in Rajasthan”, stated that the Indian Council of Medical Research (ICMR) had sequenced 5 Zika virus strains collected from Jaipur to determine genetic mutations that may lead to foetal microcephaly and high transmissibility related to the infection. The press release claimed that known mutations linked to microcephaly were not present in the Zika virus strain that had affected Rajasthan.
This article will examine the aforementioned claim made in the MoHFW press release
Claims
The ministry suggested that the results from this sequencing did not find any ‘known mutations’ linked to foetal microcephaly and high transmissibility. Thereby, the government is suggesting that:
- The Zika virus strain from India does not contain the microcephaly causing mutation
- The outbreaks is contained within small areas, thereby reducing the required precaution for pregnant women in India despite the warnings from the Centers for Disease Control and Prevention (CDC) in USA
Fact-Check
Known Mutations Linked to Microcephaly
A study in 2017 by Yuan et al in the Institute of Genetics and Developmental Biology, Beijing, China, showed that ‘S139N’ gene mutation in the genetic material of Zika virus was responsible for increased virulence and increased damage to brain cells leading to microcephaly in new-borns. However, strains lacking the mutation also damaged neural cells. This study was performed on cells in the laboratory and gives little insights into human infection. This has been falsely interpreted by the ICMR to say that strains carrying S139N mutation are solely responsible for microcephaly.
Additional studies suggest that strains of Zika strains without these mutations can cause birth defects. For example, a 2018 study from Thailand shows that even in the absence of S139N mutation, cases of microcephaly were reported.
Dr Nathan Grubaugh, Assistant Professor, Yale School of Public Health has been involved with Zika epidemic studies of Brazil and US. He spoke to Alt News and expressed deep concerns regarding the policies implemented based on ‘known mutations.’ He stated that, “There is no evidence stating S139N is responsible for 100% of the microcephaly cases. The available lab evidence suggests that any Zika virus strain may produce birth-defects. We should treat all strains as equally dangerous until further research says otherwise”. He has expressed his thoughts in details in his articles in Cell Press Review and The Hindu. This sentiment was shared by other scientists, like Scott C. Weaver, a microbiologist at the University of Texas, who worked on the Brazilian outbreak. He said “It is still too early to conclude that any particular strain cannot cause microcephaly.”
The National Institute of Virology (NIV), Pune studied the Zika strains from 10 human serum samples from Jaipur, Rajasthan, published in Infection, Genetics and Evolution. In contrast to the Ministry of Health and Family Welfare’s claim, the authors from NIV clearly state that although no S139N mutations were seen in the tested strains, it cannot be ruled out that the present strains of Zika cannot cause birth defects and large outbreaks and should be treated as such. .
Thus, expert opinions and various research data from India and abroad, suggest that the press release that claims that, there are no known microencephaly causing mutations in the virus found in India, is misinformed. This is more dangerous as the perception of this misinformation has been the basis of formatting policy to protect and educate pregnant women travelling in the areas in India where the Zika virus outbreaks have been found.
Zika virus outbreak is contained to small areas
The climate in India is conducive to the transmission of diseases by the Aedes Aegypti mosquito which is responsible to the spread of Zika, especially during the months with rainfall. Two outbreaks of Zika have been detected in India in September-October 2018. There were 154 cases in Rajasthan and 127 cases in Madhya Pradesh. The Centers for Disease Control and Prevention (CDC) in USA, had issued a warning and advised pregnant women to avoid travelling to India. However, the Government of India sent a rebuttal to CDC to withdraw or modify this alert as the outbreaks have been contained within small areas.
The extent of Zika outbreak and transmission cannot be predetermined since 4 out of 5 individuals infected with Zika do not show any symptoms and can transmit the virus. A surveillance that depends on reported cases will not be able to identify infected persons who do not show symptoms. It is not possible to say the cases were localised since most of the cases are undetected.
A 2017 paper by Siraj et al predicts that a Zika epidemic could cause more than 450 million infections in India, more than six-fold of any other country. Hence, more aggressive strategies of diagnosis, surveillance and community mobilization education, especially to pregnant women are needed.
Secondly, on one hand, the Government is downplaying the risks of Zika in India, but on the other pregnant women are being advised for abortion. In at least 2 cases, the officials advised Zika infected pregnant mothers to undergo abortion has been reported in DownToEarth.
The protocols laid down by WHO for the monitoring Zika infected pregnant women are based on ultrasound and diagnosing for microcephaly. These do not include advice for abortion. As Nathan Grubaugh has commented, clinicians advising for abortions based on Zika infection is unheard of in the rest of the world and is appalling.
Conclusion
Thus, the press release by the Ministry of Health and Family Welfare, the mention of lack of ‘known mutations’ for microcephaly is based on misrepresentation of the scientific studies conducted on the genetic material of the virus. It is inconclusive to say that a mutation linked with the most dangerous symptom of the infection, i.e. birth defects of head size, do not exist in the type of Zika virus in India.
Moreover, there is not sufficient evidence to say whether the Zika is contained in small areas as mentioned in the rebuttal to the CDC. It is likely that the extent of the outbreak goes undetected since the majority of infections do not exhibit any symptoms.
The ministry of health and family welfare should responsibly interpret the scientific studies emerging on the Zika virus and take appropriate measures to raise awareness about the disease.